Using Cesium-131 for Lung cancer
Customized individual cancer treatment.
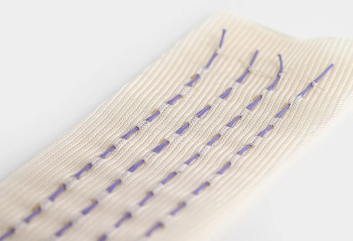
Cesium-131 Brachytherapy mesh provides conformal radiation to surgically managed patients with Non Small Cell Lung Cancer.
Brachytherapy is an established method to deliver a highly targeted dose of radiation therapy to soft tissue tumors. The procedure has become an accepted treatment for prostate cancer; however adoption of the procedure for other cancers has been slower. One opportunity where brachytherapy may provide additional benefit in the treatment of lung cancer, which is the number one cancer killer in the United States, killing more than the next three (colon, breast and prostate) cancers combined.
Cesium-131 mesh has shown promise in the treatment of certain types/stages of lung cancer.
The current experience with brachytherapy in the treatment of lung cancer has been limited as there are limited commercially available products. However, Cesium-131 mesh has shown promise in the treatment of certain types/stages of lung cancer.
There are two primary types of lung cancer: Small Cell Lung Cancer (SCLC) and Non Small Cell Lung Cancer (NSCLC). NSCLC is the most prominent, representing 80-85% of diagnoses. The main challenge with lung cancer and the reason that it is so deadly is that because it is typically asymptomatic in early stages, it is not diagnosed until it is more advanced and has spread beyond its initial site.
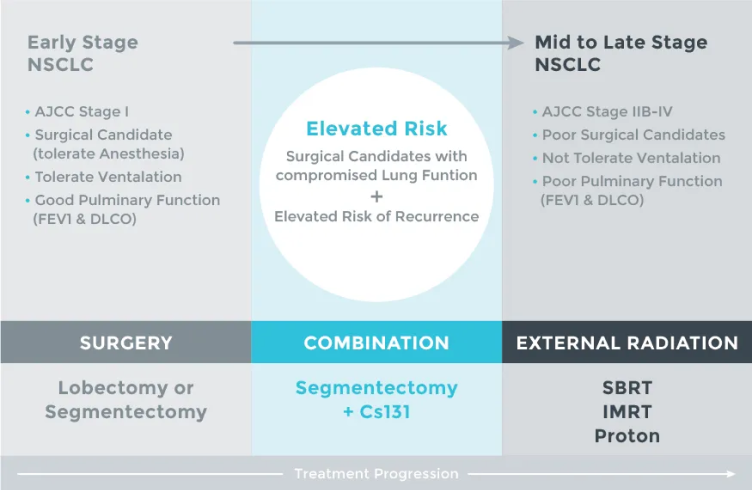
The main treatment for NSCLC is surgery, with the type of surgery dependent on the size and location of the tumor, and the patient tolerance for the procedure. The gold standard is a lobectomy where the entire lobe where the primary tumor is located is surgically removed. Variations of lung surgery include a pneumonectomy where the entire lung is removed and a segmentectomy or wedge resection, where only a portion of a lobe is removed. Other potential treatments include external radiation and targeted ablation techniques.
However, even as surgery is the gold standard, “more than 20% of patients who are diagnosed with stage I or stage II NSCLC do not undergo operation.” This may be due a variety of reasons, including poor cardiopulmonary function that compromises the overall health of the patient. One drawback of a lobectomy is its potential impact on pulmonary function, which would further stress patients who present with poor functionality. These patients may benefit from less aggressive surgical treatment, such as segmentectomy.
Cesium-131 Brachytherapy mesh provides conformal radiation to surgically managed patients with Non Small Cell Lung Cancer.
- Cesium-131 implants reach 90% of prescription does in 33 days. Six times faster than the Iodine-125 product used in historical studies.
- Cesium-131 has delivered 99.8% of the prescription dose in 90 days when the bioabsorable sutures and mesh begin to break down.
Those patients who are not candidates for lobectomy should consider, with their physicians, a sub-lobar resection wedge resection (WR) or segmental resection with brachytherapy. To compensate for the less extensive surgical resection, brachytherapy has been combined with WR to achieve results equivalent to lobectomy. In reported retrospectives studies WR with brachytherapy report excellent local control (LC) rates in early stage lung cancer.
Further information
More information on non-small cell lung cancer treatments. Visit www.cancer.gov
Want to know more about the versatility of Cesium-131
Learn moreQuestions?
Do you have questions? We can help with any issues you may have
Contact us“WR plus Cesium-131 is an excellent treatment option for patients with early stage non-small cell lung cancer that are not candidates for lobectomy. For high-risk WR we favor use of Cesium-131 brachytherapy.”
Bhupesh Parashar, MD
Analysis of stereotactic radiation vs wedge resection vs wedge resection plus Cesium-131 brachytherapy in early stage lung cancer., Brachytherapy 14 (2015) 648-654
References
United States Brief Statement
Cesium-131 brachytherapy seeds are indicated for the treatment of malignant disease(e.g., head and neck, eye, brain, breast, prostate, etc.) and may be used in surface, interstitial, and intra cavitary applications for tumors with known radio sensitivity. The seeds may be used as a primary treatment or in conjunction with other treatment modalities, such as external beam radiation therapy, chemotherapy or as treatment for residual disease after excision of primary tumors. Contraindications: As with other brachytherapy sources, treatment of tumors in generally poor condition (e.g. ulcerated) is not recommended with Cesium-131 brachytherapy seeds due to the potential for source migration. Prior to use, please reference the Cesium-131 Instructions for more information on indications, contraindications, warnings, all precautions, and adverse events.
Caution: Federal law restricts this device to sale by or on the order of a physician.